Intratympanic Injection: The Breakthrough Treatment for Sudden Hearing Loss and Tinnitus
Sudden hearing loss can strike anyone at any time, leaving patients bewildered and desperate for a solution. Traditional oral steroids often come with a host of side effects, and the window for effective treatment is alarmingly short—just 72 hours. Enter intratympanic injection, a minimally invasive procedure that delivers medication directly to the middle ear, bypassing the digestive system and maximizing therapeutic impact. This blog dives deep into how intratympanic injections work, who can benefit, and why they’re becoming the gold standard for treating sudden hearing loss, Meniere’s disease, and refractory tinnitus.
What Is an Intratympanic Injection?
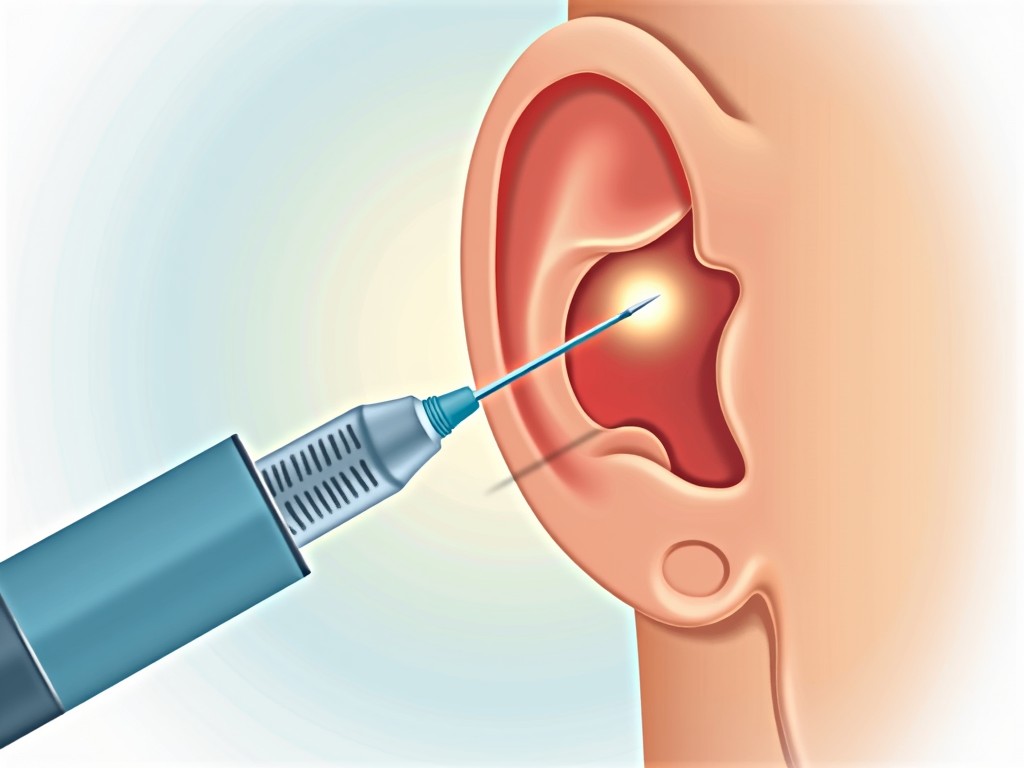
An intratympanic injection is a targeted delivery of medication through the eardrum into the middle ear. Using a fine, dental‑style needle, a clinician administers drugs—most commonly corticosteroids or gentamicin—directly into the tympanic cavity. Because the medication is applied locally, it achieves high concentrations in the inner ear while minimizing systemic exposure.
Key Advantages
- Rapid onset – The drug reaches the inner ear within minutes, crucial for the 72‑hour treatment window in sudden hearing loss.
- Reduced side effects – No oral steroids mean no gastrointestinal upset, weight gain, or blood‑pressure spikes.
- High local concentration – The drug bypasses the blood‑labyrinth barrier, allowing therapeutic levels that oral dosing cannot achieve.
- Minimal discomfort – The eardrum is numbed with lidocaine spray; patients typically feel no pain during the procedure.
- Quick recovery – The tiny puncture in the eardrum heals almost instantly, and patients can resume normal activities within 10 minutes.
Who Can Benefit?
While intratympanic injections are most famous for treating sudden sensorineural hearing loss (SSHL), they’re also effective for several other ear disorders:
- Sudden Hearing Loss – The only proven pharmacologic treatment is corticosteroids; intratympanic delivery matches oral efficacy with fewer systemic risks.
- Meniere’s Disease – When vertigo is refractory to oral medications, intratympanic gentamicin can reduce inner‑ear fluid and control episodes.
- Refractory Tinnitus – For patients whose tinnitus does not respond to sound therapy or oral drugs, intratympanic steroids or gentamicin can provide relief.
- Chronic Otitis Media with Effusion – Steroid injections can reduce inflammation and improve hearing thresholds.
How the Procedure Works
The intratympanic injection is performed in a clinical setting under local anesthesia. Here’s a step‑by‑step overview:
- Preparation – The patient is seated and the ear is cleaned. A lidocaine‑containing spray numbs the eardrum.
- Microscopic Guidance – A surgical microscope provides a magnified view of the tympanic membrane.
- Injection – A fine, dental‑style needle is carefully inserted through the eardrum into the middle ear. The medication is slowly injected.
- Post‑procedure – The patient rests for about 10 minutes. A tiny puncture in the eardrum seals itself within hours.
- Follow‑up – Depending on the condition, multiple injections may be scheduled over several weeks.
Safety and Side Effects
Because the drug is delivered locally, systemic side effects are rare. Common, mild side effects include:
- Temporary ear fullness or pressure
- Minor ear pain (usually resolved within minutes)
- Transient taste disturbance from the Eustachian tube
Serious complications are exceedingly uncommon but can include:
- Perforation of the eardrum (usually self‑healing)
- Infection (prevented with sterile technique)
- Inner‑ear damage (only with high doses of gentamicin)
Clinical Evidence Supporting Intratympanic Injections
Numerous randomized controlled trials and meta‑analyses confirm that intratympanic steroids are as effective as oral steroids for SSHL, with the added benefit of fewer systemic adverse events. For Meniere’s disease, intratympanic gentamicin has shown significant vertigo control in patients who failed medical therapy. Tinnitus studies demonstrate that intratympanic steroids can reduce perceived loudness and improve quality of life in a subset of patients.
Frequently Asked Questions
1. How many injections are needed?
Most protocols involve 1–3 injections per ear, spaced 1–2 weeks apart. The exact number depends on the underlying condition and the patient’s response.
2. Is the procedure painful?
After lidocaine numbing, patients report little to no pain. Some may feel a brief pressure sensation.
3. Can I drive after the injection?
Yes, most patients can resume normal activities immediately. However, avoid swimming or submerging the ear for 24 hours.
4. Are there any contraindications?
Active ear infection, severe tympanic membrane perforation, or known allergy to the medication are contraindications. Your clinician will assess suitability before proceeding.
Conclusion
Intratympanic injection represents a paradigm shift in otologic therapy. By delivering medication directly to the middle and inner ear, it maximizes therapeutic benefit while minimizing systemic risks. Whether you’re battling sudden hearing loss, Meniere’s disease, or stubborn tinnitus, this minimally invasive procedure offers a promising path to recovery. If you suspect a sudden hearing change or chronic ear symptoms, consult an otolaryngologist to explore whether intratympanic injection is right for you.